| CAS NO: | 83-43-2 |
| 包装 | 价格(元) |
| 10mM (in 1mL DMSO) | 电议 |
| 100mg | 电议 |
| 250mg | 电议 |
| 500mg | 电议 |
| 1000mg | 电议 |
| Cas No. | 83-43-2 |
| 别名 | 甲泼尼龙; U 7532 |
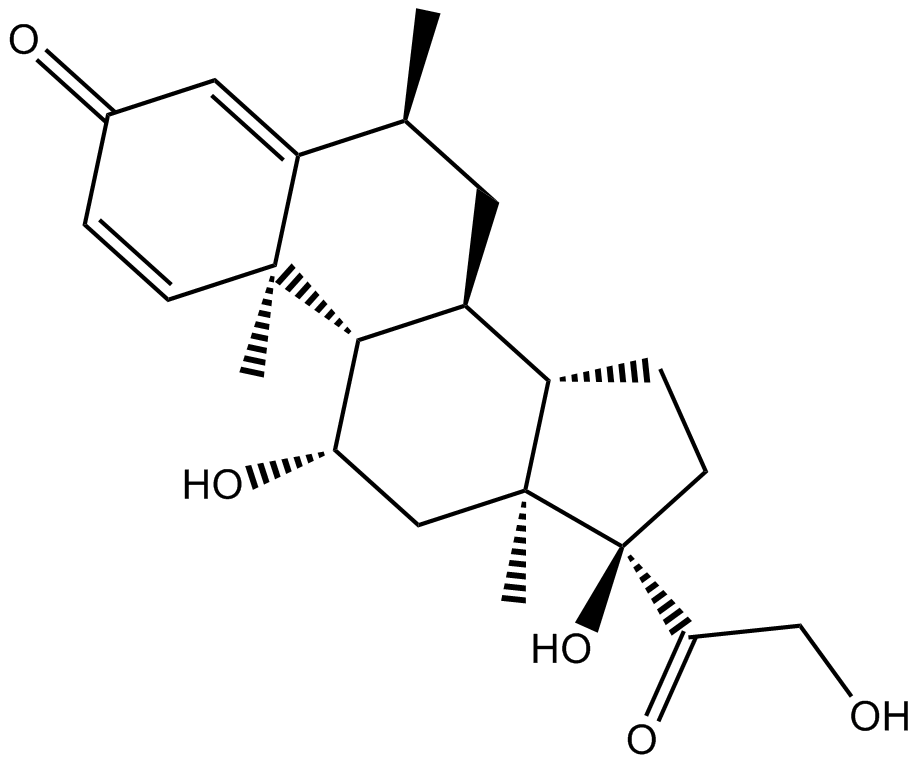
| 化学名 | (6S,8S,9S,10R,11S,13S,14S,17R)-11,17-dihydroxy-17-(2-hydroxyacetyl)-6,10,13-trimethyl-7,8,9,11,12,14,15,16-octahydro-6H-cyclopenta[a]phenanthren-3-one |
| Canonical SMILES | CC1CC2C3CCC(C3(CC(C2C4(C1=CC(=O)C=C4)C)O)C)(C(=O)CO)O |
| 分子式 | C22H30O5 |
| 分子量 | 374.48 |
| 溶解度 | ≥ 15.35 mg/mL in DMSO, ≥ 9.5 mg/mL in EtOH with ultrasonic |
| 储存条件 | 4°C, protect from light |
| General tips | For obtaining a higher solubility , please warm the tube at 37 ℃ and shake it in the ultrasonic bath for a while. |
| Shipping Condition | Evaluation sample solution : ship with blue ice All other available size: ship with RT , or blue ice upon request |
| 产品描述 | Methylprednisolone is a synthetic glucocorticoid receptor agonist, used to achieve prompt suppression of inflammation. In vitro: Methylprednisolone (2-10 mg/kg) significantly inhibited TNF production. High doses of methylprednisolone (50 mg/kg) increased LPS-induced IL-10 levels. Methylprednisolone (0.01-100 μg/ml) increased the biosynthesis of IL-10 in LPS-activated mouse peritoneal macrophages [1]. In WG patients and controls, methylprednisolone (MP) down-regulated the spontaneous and the staphylococcal enterotoxin B (SEB)-induced release of chemokines from peripheral blood mononuclear cells (PBMC)[2]. Treatment with 0.25 mM methylprednisolone inhibited acantholysis in skin cultures directly [3]. In vivo: Methylprednisolone (30 mg/kg, i.v.) given immediately after SCI reduced TNF-α expression by 55% (P<0.01) and NF-kB binding activity. Methylprednisolone suppressed the Post-traumatic inflammatory activity caused by TNF-alpha-NF-kB cascade[4]. Intravenously administration of MP (30 mg/kg) reduced the number of ED1-positive cells by 82% in the rostral cord stump and 66% in the caudal stump. In the adult rat, MP administration shortly after spinal cord transection resulted in a long-term reduction of ED1-positive cells and spinal tissue loss, reduced dieback of vestibule spinal fibres, and a transient sprouting of vestibule spinal fibres near the lesion at 1 and 2 weeks post-lesion. MP treatment also significantly reduced the tissue loss in both cord stumps at 2, 4 and 8 week post-injury[5]. Cllinical trials: In patients with acute spinal cord injury diagnosed in National Acute Spinal Cord Injury Study (NASCIS) centers within 8 hours of injury, methylprednisolone treatment for 48 hours improved motor recovery at 6 weeks (P= 0.09) and 6 months (P= 0.07) after injury[6]. In patients with acute spinal-cord injury, methylprednisolone (30 mg/kg) followed by infusion at 5.4 mg/kg/hour for 23 hours improved neurologic recovery. Among patients treated with methylprednisolone (30 mg/kg), mortality at 14 days was significantly increasedsecondary infection[7]. Methylprednisolone has entered clinical trials in patients with severe renel vasculitis and lupus nephritis. References: |
 m.cnreagent.com
m.cnreagent.com